Patient Positioning:
- Supine position on a large vacuum cushion. The use of the cushion eliminates the need for additional supports
- Padding for extremities and pressure-prone areas
- A protective bar is recommended to shield the patient from robotic arms
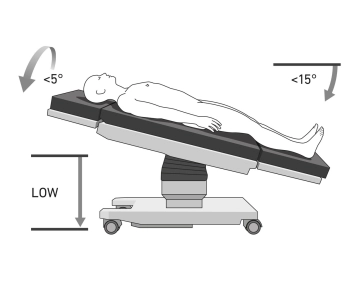
- After trocar placement, tilt the operating table to:
- 15° Anti-Trendelenburg
- 5° Right tilt (tilt right)
- The robotic arms are docked to the patient
Cautions:
- Ensure secure positioning due to the risk of abdominal wall injuries if the patient slips while docked to the robot
- Verify the vacuum cushion for leaks before sterile draping
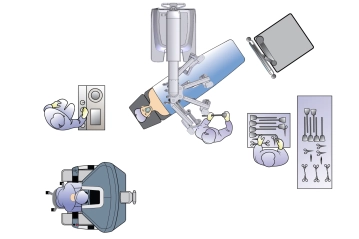
Setup Details:
- Surgeon: Operates from the robotic console with visibility of both the patient and the table assistant
- Table Assistant: Positioned on the patient’s right
- Anesthesiologist: At the patient’s head
- Patient Cart: Approaches the patient from the left side
- Scrub Nurse: Positioned to the right of the table assistant