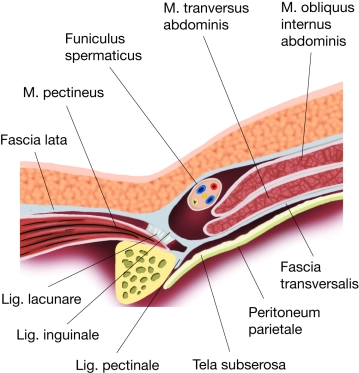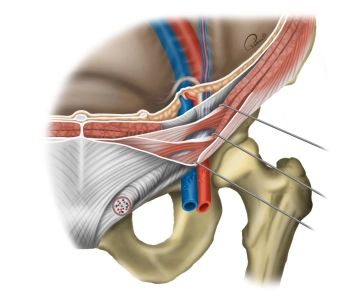
The inguinal region (transition between the anterior abdominal wall and the lower extremity) has several weak points through which a hernial sac with or without contents can protrude through the abdominal wall (women are more prone to femoral hernias, men to inguinal hernias). Below the inguinal ligament, the inguinal canal is divided into two compartments by a division of the inguinal ligament (arcus iliopectineus): the lacuna vasorum and the lacuna musculorum.
Lacuna vasorum
- Located next to the pubic bone, it serves as the passageway for the external iliac artery and vein (→ femoral artery and vein, arrangement: artery lateral to the vein). The femoral branch of the genitofemoral nerve passes through it laterally. Caudally medial, the deep inguinal lymph nodes (Rosenmüller) are found here. The lacuna vasorum represents the internal hernial orifice for femoral hernias (through the femoral septum next to the femoral vein).
Lacuna musculorum
- Located lateral to the lacuna vasorum, it serves as the passageway for the psoas major muscle and iliacus muscle (together = iliopsoas muscle) as well as for the femoral nerve and lateral femoral cutaneous nerve (cranially).