
Perform median laparotomy from xiphoid down to symphysis, carrying the incision to the left of the umbilicus.
-
Laparotomy
![Laparotomy]()
Soundsettings -
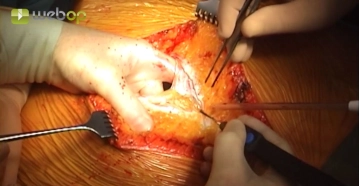
Opening the retroperitoneum
![Opening the retroperitoneum]()
Soundsettings Open the retroperitoneum to the right of the palpable aorta and coagulate any small visible vessels prior to transection. Locate the inferior mesenteric vein.
Tip:
An incision midway over the aorta may result in more severe bleeding from small, anteroaortic vessels, and there is the risk of inadvertent injury to the inferior mesenteric artery. Incisions carried more to the right of the aorta avoid these risks.
-
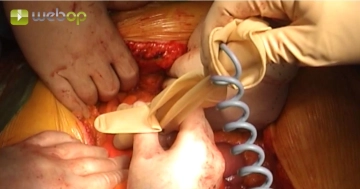
Locating the superior mesenteric artery
![Locating the superior mesenteric artery]()
Soundsettings Locate the superior mesenteric artery in the course of the mesenteric axis using a Doppler ultrasound probe.
Tip:
Sometimes it is difficult to palpate the stenosed/occluded vessel, especially if the mesentery is quite fatty. As demonstrate din the video clip, it is quite helpful in such cases to locate the artery with a Doppler ultrasound probe prior to incision of the mesentery.
-
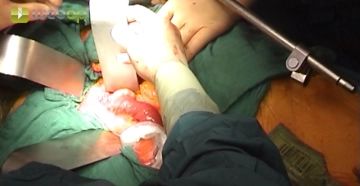
Evenetration of the small intestine and establishing the surgical field with the abdominal wall retractor system
![Evenetration of the small intestine and establishing the surgical field with the abdominal wall retractor system]()
Soundsettings Displace the small intestine outside the abdominal cavity to the right and enclose it in a plastic bag. Displace the transverse colon and the greater omentum into the upper abdomen, cover them with a moist abdominal towel and kepp them there with a blade of the retractor system. Cover th mesentery of the descending colon with a moist abdominal towel and displace it to the left with another blade of the retractor system.
Tip:
Placing the small bowel in a plastic bag or wrapping it in plastic sheeting ensures that the bowel remains moist and does not sustain serosal lesions. This can also help prevent postoperative adhesions.
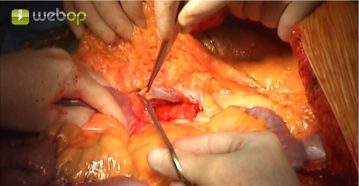
Exposing the superior mesenteric artery
Incise the mesenteric root inferior to the colon and expose the superior mesenteric artery, which i
Incise the mesenteric root inferior to the colon and expose the superior mesenteric artery, which i
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.32 / module
US$51.88/ yearly payment
vascular surgery
Unlock all courses in this module.
US$8.64
/ month
US$103.80 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.