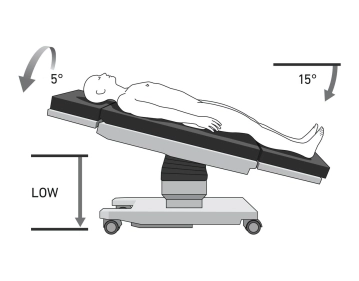
The patient is positioned in supine position on the large vacuum cushion. The left arm can be positioned separately. The use of the cushion eliminates the need for any additional supports.
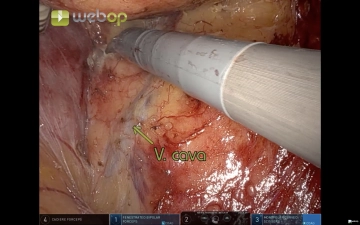
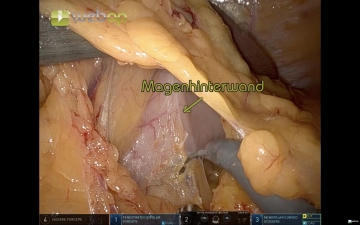
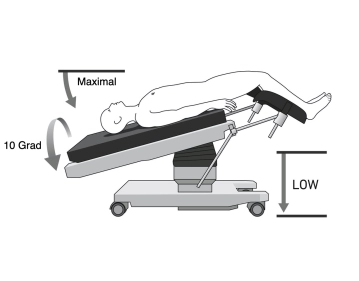
Initially, for the Artery First Approach, the patient is positioned in maximum head-down and right lateral position. From step 5 (opening of the bursa), the patient is then positioned slightly head-up and slightly in right lateral position.
Important: The positioning is of particular importance due to the docking of the patient to the robot's manipulator. Unless a coupled table (so-called Table-Motion function) is available, the arms must be undocked before each table movement. There is also a risk of injury if the patient slips.
Note: Vacuum cushions can have leaks. Check again before sterile draping.
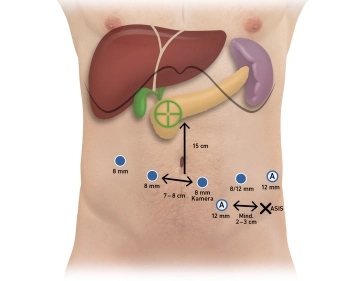
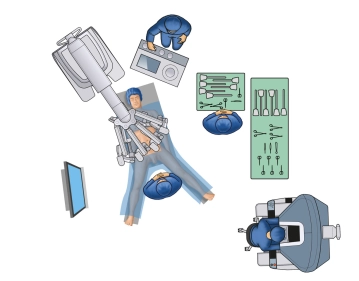
The surgeon ideally sits at the console with the ability to look at the patient and the table assistant. The surgical robot (Patient Card) is approached to the patient from the cranial side in the X-System. In the Xi, the Patient Card can be variably approached to the patient, for example, directly from the right. The table assistant stands or sits on the left side of the operating table. Anesthesia is located at the head of the patient, and the scrub nurse is positioned to the right of the patient's legs with the table over the legs.