The VAC stent combines elements of both a self-expanding metal stent and endoscopic vacuum therapy in a single instrument.
The nitinol stent is fully covered with a silicone membrane that is impermeable to liquids and gases and is encased by a polyurethane sponge cylinder.
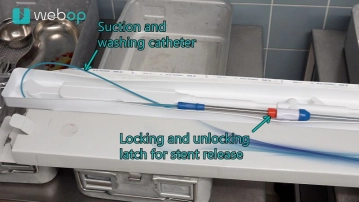
A 2.5 m long polyurethane suction catheter with a diameter of 10 French and a removable Luer-Lock connector is embedded in the open-pore sponge. After transnasal redirection, it connects to an adjustable vacuum pump. The ends of the covered stent are in contact with the intestinal wall and seal the lumen.
The metal stent has a body length of 50 mm and an expanded diameter of 14 mm, as well as two dumbbell-shaped ends, each 10 mm long, expanding to a diameter of 30 mm. This results in a total stent length of 70 mm. The stent body contains six radiopaque titanium markers to assist positioning under fluoroscopic control. The sponge is attached to the stent body with a suture thread.
The stent is delivered pre-assembled on a 1 m long over-the-wire introduction system.
The Esophagus-VACStent® is available in only one size and is CE-certified (Conformité Européenne).