Since spontaneous healing of rectovaginal fistulas is rare even after the creation of a stoma, and conservative measures almost never lead to healing, the only sufficient therapy is surgical fistula repair.
Surprisingly, many patients present with fistulas that have existed for many years, which seems to be due to a minor or nonexistent level of distress and, naturally, also to shame. It is not uncommon for the presentation for fistula repair to occur at the urging of the partner or family, and occasionally the diagnosis is made incidentally, for example, during the diagnosis and treatment of other diseases.
Decisive for the indication for surgical fistula repair are a corresponding level of distress, recurrent infections, and possibly existing continence disorders. If there is no significant distress and/or the fistula is asymptomatic, the indication for surgery should be made with caution.
When is the ideal time for fistula correction?
With corresponding distress, rectovaginal fistulas should be repaired as quickly as possible. However, the condition of the affected tissue areas plays a crucial role in choosing the timing of the operation.
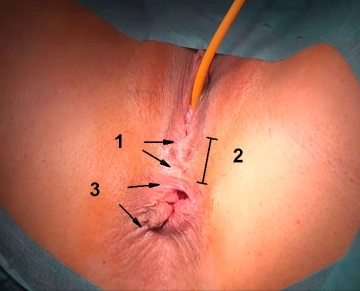
Before starting surgical measures, any existing inflammatory processes such as induration or inflammation must have largely subsided. If a fistula becomes symptomatic in the context of an abscess formation, one initially limits to an abscess incision and marking of the fistula with a vessel loop before aiming for fistula repair in a further step. The subsiding of inflammatory reactions can be supported by regular sitz baths, irrigation, possibly also debridement, 10-14 days of oral broad-spectrum antibiotics, and a low-fiber diet.
If the fistula is causally due to perineal trauma, for example, as a complication of the primary reconstruction of a higher-grade perineal tear during vaginal delivery, at least 10-12 weeks should be waited after the triggering event.
When is the placement of a protective, temporary stoma indicated?
The placement of a protective stoma is advisable for all fistula types with pronounced local inflammatory and scar changes, wide tissue defects, and anorectal incontinence requiring complex sphincter reconstruction. The so-called "complicated fistula disease" includes:
- Multiple fistula openings present
- Horseshoe-shaped or suprasphincteric fistula forms
- Wide fistula openings, which usually entail a difficult closure technique (e.g., gracilis interposition)
- Pronounced inflammatory perineal and perianal changes
- Crohn's fistulas
- Radiogenic fistula
- Severe obstetric injuries such as perineal loss
If a protective stoma is required, detailed counseling of the affected patient is mandatory not only by the surgeon but also by a stoma therapist, as well as the referral to self-help groups.
The reversal of a protective stoma should occur no earlier than 3 months after successful fistula repair.
Special case: Rectovaginal fistula and Crohn's disease
Fistulas that arise in the context of Crohn's disease have an extremely poor prognosis with a recurrence rate of over 50%. Fistula repairs during an acute flare should be avoided regardless of the location of the affected intestinal segment. Surgical measures must be postponed until the flare subsides, and the indication for the placement of a protective stoma should be made generously.