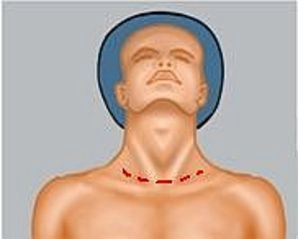
Collar Incision in Pronounced Skin Emphysema
1.1 Complications due to Positioning
To improve organ exposure, patients are often placed in extreme positions during laparoscopic procedures, which is why superficially running, long nerves can be compromised during positioning. Particularly at risk are:
- N. peroneus
- N. femoralis
- N. ulnaris
- Brachial plexus
Prophylaxis
- padded shoulder supports in anticipated head-down position
- in the lithotomy position, the leg holders in the area of the fibular heads should be additionally padded with gel cushions
- with arms positioned alongside, these should be additionally padded in the elbow area and loosely fixed to the body in pronation position
- abducted arms should be placed on a padded splint and not abducted more than 90°
1.2 Complications due to Trocar Insertion
Insertion of trocars, especially the first trocar, can lead to injuries to hollow organs and vessels, which in many cases results in prompt conversion to laparotomy for safe assessment and treatment of the injury. In particular, the assessment of vascular injuries that occur retroperitoneally is hardly possible laparoscopically. Even if an accidental bowel injury should be manageable laparoscopically, the possibility of further intra-abdominal injuries that are not recognizable at first glance must also be considered.
1.3 Complications due to Pneumoperitoneum
The pneumoperitoneum can trigger numerous pathological changes at hemodynamic, pulmonary, renal, and endocrine levels. Depending on the intra-abdominal pressure, the type of anesthesia, the ventilation technique used, and underlying diseases, serious complications may occur due to inadequate anesthesia management.
1.3.1 Cardiovascular Complications
- Arrhythmias
- Cardiac arrest
- Pneumopericardium
- Hypo-/Hypertension
1.3.2 Pulmonary Complications
- Pulmonary edema
- Atelectasis
- Gas embolism
- Barotrauma
- Hypoxemia
- Pneumothorax/-mediastinum
Immediate Measures
- Release the pneumoperitoneum
- if the complication cannot be managed by anesthesia: possibly convert to open procedure or abort the intervention
Special Case: Extreme Subcutaneous Skin Emphysema
In up to 3% of all laparoscopies, a collar skin emphysema occurs, which untreated can lead to impending compression of the airways and secondarily to a pneumothorax and pneumomediastinum and requires a collar incision to release the CO2. If there are no ventilation problems with a CO2 pneumothorax, one can initially wait, as the CO2 in the thorax is quickly resorbed. In case of ventilation problems or an extensive capnothorax, thoracic drainage is indicated. Particularly affected are older patients due to the flaccid tissue.
1.4 Procedure-Specific Complications
The procedure-specific complications of laparoscopic liver resection correspond to those of the open technique. If they cannot be managed laparoscopically, conversion to laparotomy should not be delayed. Proceed then depending on the complication as described below:
1.4.1 Bleeding
Arterial Bleedings
- Can occur during dissection of the hepatic hilum, are usually well manageable
- Due to the risk of injury to bile duct structures and further vascular injuries, bleedings in the hepatic hilum should not be blindly sutured, instead successive free preparation and targeted treatment
- Arterial vessel leaks: direct suture with Prolene® 5-0 or 6-0 or clip
- In accidental transection of a main artery, reconstruction is mandatory, reanastomosis, possibly using a saphenous vein interponate
Venous Bleedings
- e.g., from the portal vein, are much more difficult to manage: under local control of the bleeding, an overview should first be obtained, then clamped proximally and possibly the vessel oversewn.
- Bleedings from the vena cava are possibly difficult to control
- In retrohepatic localized bleedings, which can occur during mobilization of the liver, the vena cava is usually not yet sufficiently exposed to clamp it tangentially. Here, only grasping and narrowing the vena cava helps, best with forceps; then free preparation of the lesion and oversewing; in this situation, it is helpful if the vena cava was previously looped infrahepatically
- In bleedings from the vena cava at the level of the hepatic vein ostia, bleeding control is often only possible by manual compression
- In difficult situations, it may be necessary to temporarily occlude the vena cava below and above the liver. For this, opening of the diaphragm at the level of the cava passage may be necessary
- Caution: there is a risk of air embolism!
Bleedings from the Liver Resection Surface
- Targeted sutures
- No deep mass sutures, they lead to necroses of the surrounding parenchyma and can result in injuries to adjacent vessels, e.g., thin-walled hepatic veins
- In diffuse bleedings: coagulation e.g. with an argon beamer
- In massive diffuse bleeding from the resection surface (usually due to coagulation disorders), temporary packing with abdominal towels may also be necessary
Prophylaxis of Intraoperative Bleedings
- Adequate access with sufficient exposure
- Generous mobilization of the liver
- Preliminary hilar ligations in anatomical lobectomies
- Intraoperative sonography with depiction of the vascular structures in the resection area
- Controlled parenchyma dissection
- Avoidance of overfilling of the venous system (low CVP)
- Careful treatment of the resection surface
Compromise of Arterial Blood Supply
- In principle, caution is advised during preparation of the hilum to avoid accidentally injuring or ligating the wrong artery. This would mean a significant complication.
1.4.2 Bile Leaks
- If gallbladder is still present: occlusion of the common bile duct and manual compression of the gallbladder with simultaneous inspection of the liver resection surface; possibly targeted suture
- If gallbladder already removed: perform a methylene blue or Lipovenös test via the cystic stump: Lipovenös or methylene blue is injected under pressure into the biliary system, so that bile leaks can be well demonstrated by the exit of white fat emulsion or the blue solution.
1.4.3 Air Embolism
- Air embolisms (in laparoscopic procedures: CO2 embolisms) can arise from unintentional or unnoticed opening of small hepatic veins, which manifests as sudden tachycardia, hypotension, arterial hypoxemia, arrhythmias, and an increase in CVP. The embolisms are favored by low or even negative CVPs.
- Avoid further entry of air by detection, clamping or oversewing of the entry site, immediate PEEP ventilation.
1.4.4 Pneumothorax
- Can occur in tumors close to the diaphragm or infiltrating → intraoperative thoracic drainage
1.4.5 Transection of the D. choledochus
- after accidental transection of the D. choledochus, if there is good blood supply to both stumps, a direct anastomosis can be performed, possibly insertion of a T-drain
- in uncertain blood supply conditions, the creation of a hepaticojejunostomy is indicated
1.4.6 Hollow Organ Injuries
- In pre-operated patients, especially after cholecystectomy or previous interventions on the stomach, adhesiolysis must be performed. Hollow organs can be injured in the process.