The functional structure of the liver rests on the portal vein ramifying into individual, completely independent subunits, the liver segments.
In the porta hepatis, the portal vein usually bifurcates into a left and right lobar branch.The outer margin of these areas is defined by Cantlie’s line, i.e., the vertical plane extending from the inferior vena cava posteriorly to the middle of the gallbladder fossa anteriorly. The right lobar branch divides into an anteromedial and posterolateral branch supplying the liver segments V/VIII and VI/VII respectively. The left lobar branch of the portal vein courses transversely to the left, continuing anteriorly as umbilical branch and terminating at the insertion of the ligamentum teres in the recessus of Rex. The left lobar branch of the portal vein gives off branches to both left lateral segments II and III, and to the median segments IVa and IVb as well. The small caudate lobeis special because it may receive sizable tributaries from the left and right lobar branch of the portal vein.
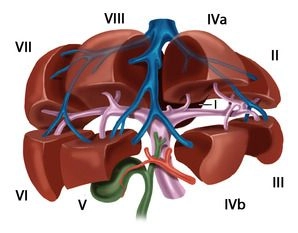
Couinaud identified eight portovenous liver segments which are numbered clockwise starting with the caudate lobe:
Segment I………………………..caudate lobe
Segments I/II/III………………… left lateral hepatic lobe
Segment IV………………………left paramedian sector (quadrate lobe)
Segments I/II/III/IV………………left lobe of liver
Segments V/VIII…………………right paramedian sector
Segments VI/VII…………………right lateral sector
Segments V/VI/VII/VIII………….right lobe of liver
Three major venous trunks traverse the liver caudocephalad; these are the right, median and left hepatic veinswhich divide the liver into a total of four hepatic sectors.The left hepatic vein almost exclusively drains the left lateral hepatic lobe, and just before its junction with the inferior vena cava it usually merges with the middle hepatic vein which courses along the cava-gallbladder line. The right hepatic vein travels between the posterolateral and anteromedial segments. The caudate lobe has its own venous drainage, the Spieghelian veins, comprising multiple small posterior veins draining directly into the inferior vena cava.
In reality, the regularity of the venous branching described by Couinaud is seen only in few cases, and there are numerous branch variants supplying areas of varying size.
The portal hila of liver segments II, III and IV are extrahepatic and can be easily exposed in the anterior section of the left umbilical fissure. The portal hila of the right liver segments are intrahepatic; while there are exceptions at times, these mostly pertain to segment VI. The anatomy of the hepatic veins is even more variable than that of the portal vein.