

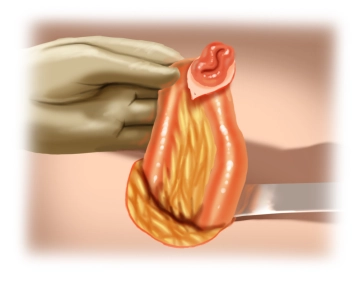
Oval incision around the stoma with a skin margin of about 2 mm wide; dissect through the subcutaneous tissue and possibly close the stoma by suture (here, fixation of the proximal limb with a stay suture for better mobilization and to avoid wound contamination with fecal content of the small intestine).
-
Skin incision
![Skin incision]()
-
Freeing and dissecting down to the fascia
![Freeing and dissecting down to the fascia]()
Free the proximal and distal limbs along their circumference from their adhesions with the subcutaneous tissue down to the fascia while keeping close to the intestine. Here, the stoma is completely freed from the fascia while carefully sparing the small bowel mesentery. Dissect the skin and subcutaneous tissue only as much as appears necessary for safe intestinal suture. Excessive dissection increases the risk of hematoma and/or infection.
-
Freeing the small intestine
![Freeing the small intestine]()
After checking with the finger that the stoma has been completely released from the fascia, the loop of the small intestine bearing the stoma can be loosely delivered through the abdominal wall.
-
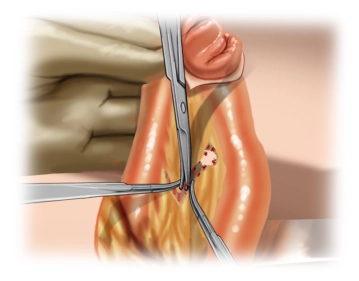
Dissecting the mesentery
![Dissecting the mesentery]()
Once the small intestine has been freed, skelettonize the mesentery of the proximal and distal limb only so far as to be able to resect the stoma section.
Comment: Some surgeons dissect the scar remaining on the intestinal wall to allow direct anastomosis. For this resect the remaining skin with scissors. Take care that the posterior wall of the intestine is spared as wide as possible. After checking that the mesentery is intact, close the intestine with an absorbable monofilament continuous submucous suture 4/0.
If the bridge of the posterior wall is too small, if vascular injury to the mesentery has impaired intestinal circulation or if the intestinal segment to be anastomosed demonstrates ischemia, a short resection of the intestinal segment with direct anastomosis is mandatory.
Since the bridge of the posterior wall is too small in the majority of cases, short resection with direct anastomosis should be regarded as standard procedure. This can be end-to-end or, as in this article, side-to-side. -
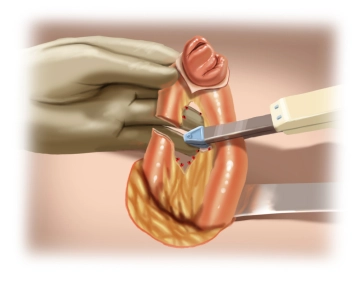
Stoma resection
![Stoma resection]()
Resect the stoma-bearing ileum segment (length: approx. 10cm). This can be done sharply (after placing soft intestinal clamps) when constructing an end-to-end anastomosis or, as here, with a stapler. This is the more expensive variant, which, apart from a small gain in time, offers no significant benefit. The decisive factor is a sufficiently wide anastomosis to avoid postoperative motility disorders and the danger of ileus.

Preparing the anastomosis
When constructing a side-to-side anastomosis grasp the ends of the intestinal limbs, place them par
When constructing a side-to-side anastomosis grasp the ends of the intestinal limbs, place them par
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
general and visceral surgery
Unlock all courses in this module.
€12.42
/ month
€149.00 / yearly payment