
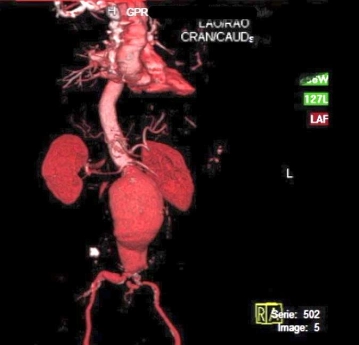
Infrarenal AAAs greater than 5 cm in diameter and aneurysmal neck angulation greater than 60° do not lend themselves to EVAR.
-
Dynamic three-dimensional spiral CT image of an infrarenal abdominal aortic aneurysm (AAA)
![Dynamic three-dimensional spiral CT image of an infrarenal abdominal aortic aneurysm (AAA)]()
Soundsettings -
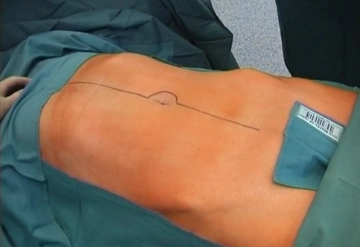
Laparotomy
![Laparotomy]()
Soundsettings Perform median laparotomy from xiphoid down to symphysis, carrying the incision to the left of the umbilicus.
Tips:
1. Maintain adequate distance from the umbilicus and do not incise the skin tangentially as this runs the risk of wound edge necrosis.
2. If the incisdion damages the cartilage of the xiphoid, it may trigger heterotopic ossification in the scar. Therefore start the incision somewhat lateral to the xiphoid.
-
3. Opening the retroperitoneum
![3. Opening the retroperitoneum]()
Soundsettings After exploring the abdomen, sweep the small intestine to the right and the transverse colon into the upper quadrants. Coagulate smaller vessels and open the retroperitoneum slightly to the right of the right iliac axis, sparing the inferior mesenteric artery (AMI) and lymphatic pad. Carry the incision to the right of the AAA. Mobilize the duodenojejunal flexure.

Dissecting the pelvic arteries and the aneurysm neck
Expose the right common iliac artery by dissecting directly on the vessel and sweep the preaortic l
Expose the right common iliac artery by dissecting directly on the vessel and sweep the preaortic l
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.33 / module
US$52.04/ yearly payment
vascular surgery
Unlock all courses in this module.
US$8.67
/ month
US$104.10 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.