
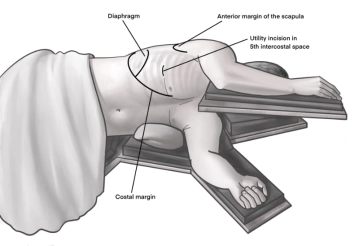
Incision of approximately 4 cm in length in the area of the anterior axillary line at the upper edge of the 5th rib to access the 4th intercostal space above. A useful orientation is often an imaginary line from the tip of the scapula to the nipple. Transection of the subcutis on the rib with the monopolar knife. Subsequently, stepwise preparation of the intercostal muscles with the monopolar knife. The pleura is opened bluntly with a finger. Palpation of the thoracic wall for adhesions and insertion of a wound protection film.
-
Access uniportal VATS right
![Access uniportal VATS right]()
-
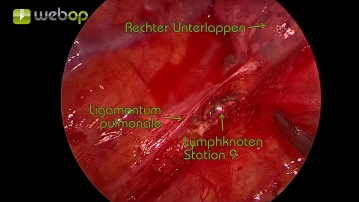
Exploration of the thorax and preparation of the pulmonary ligament
![Exploration of the thorax and preparation of the pulmonary ligament]()
Soundsettings Initially, the thorax is explored for macroscopically suspicious lesions and adhesions. Subsequently, the preparation of the pulmonary ligament for lung mobilization is begun. The preparation is extended cranially, paraesophageal at the dorsal hilum. During this process, the lymph nodes of stations 8 and 9 (according to IALSC = International Association for the Study of Lung Cancer) are removed.
-
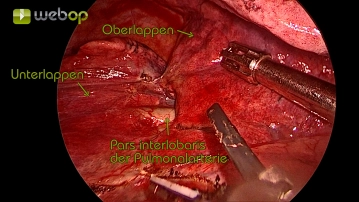
Preparation of the interlobium between the upper, middle, and lower lobes
![Preparation of the interlobium between the upper, middle, and lower lobes]()
Soundsettings Careful opening of the interlobar visceral pleura and exposure of the interlobar part of the pulmonary artery.
Preparation of the pulmonary artery with visualization of the segmental artery A6
In preparation for the resection of the segmental artery A6 with the stapling device and for clear
In preparation for the resection of the segmental artery A6 with the stapling device and for clear
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.10
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.23 / module
US$50.80/ yearly payment
thoracic
Unlock all courses in this module.
US$8.46
/ month
US$101.60 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.