
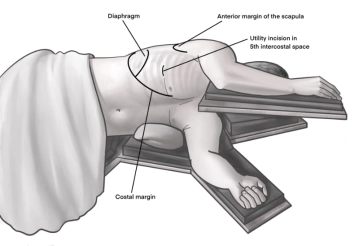
Incision of approximately 4 cm in length in the area of the anterior axillary line at the upper edge of the 5th rib to access the 4th intercostal space above. As a guide, an imaginary line from the tip of the scapula to the nipple is often helpful here. Transection of the subcutis on the rib with the monopolar knife. Subsequently, stepwise preparation of the intercostal muscles with the monopolar knife. The pleura is opened bluntly with fingers. Palpation of the thoracic wall for adhesions and insertion of a wound protection film.
-
Access uniportal VATS right
![Access uniportal VATS right]()
-
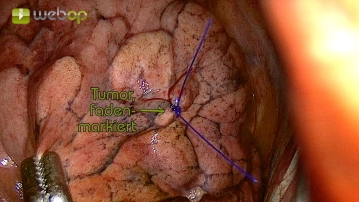
Exploration and tumor marking
![Exploration and tumor marking]()
Soundsettings First, the exploration of the situs and palpation of the lung is performed. If the nodule described in the imaging can be reliably palpated and no further findings (such as pleural carcinomatosis) are observed, marking the tumor with a suture or sterile pen during the subsequent parenchymal resection is very helpful to ensure an adequate safety margin.
-
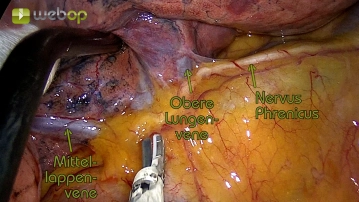
Preparation of the upper lobe vein
![Preparation of the upper lobe vein]()
Soundsettings In the case presented here, a very clear anatomy of the lung hilum is already evident before dissection. Initially, the pleural covering is incised. Care must be taken to preserve the phrenic nerve. Subsequently, the preparation of the upper pulmonary vein is predominantly blunt. In the case of planned segmental resection, it is not circumferentially dissected free but followed peripherally until the branching into individual branches is clearly recognizable. Accurate assignment of the venous branches to the segments is often only reliably possible later in the operation, so dissection is performed at a later stage.
-
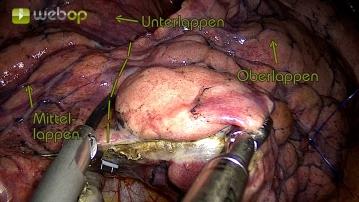
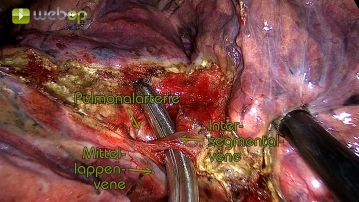
Dissection of the minor fissure
![Dissection of the minor fissure]()
Soundsettings The fissure between the upper and middle lobes is at most suggested. Initially, stepwise dissection with the ultrasonic scissors is performed until the interlobar part of the pulmonary artery is exposed. An intersegmental vein, clearly extending from the middle lobe vein into segment 3, is circumferentially dissected.
- Note:
The parenchyma of the middle lobe remaining in situ must later be visceralized by suturing to prevent a persistent parenchymal fistula postoperatively. In this process, the lung parenchyma is sutured in such a way that the resection site is covered with lung tissue and intact visceral pleura. (See step 14)
-
Dissection of the intersegmental vein
![Dissection of the intersegmental vein]()
Soundsettings The previously circularly dissected intersegmental vein can then be transected using the ultrasonic shears while placing titanium clips. The remaining parenchymal bridge underneath is also resected. Care must be taken to preserve the middle lobe vein and the pars interlobaris of the pulmonary artery.
Preparation of the interlobar part of the pulmonary artery
Subsequently, the pars interlobaris of the pulmonary artery is further dissected. It is crucial to
Subsequently, the pars interlobaris of the pulmonary artery is further dissected. It is crucial to
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.30
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$4.32 / module
US$51.88/ yearly payment
thoracic
Unlock all courses in this module.
US$8.64
/ month
US$103.80 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.