
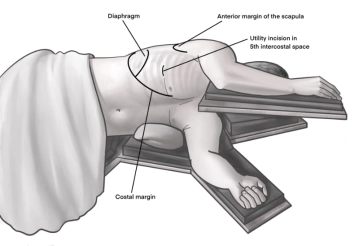
Incision of approximately 4 cm in length in the area of the anterior axillary line at the upper edge of the 5th rib to access the overlying 4th intercostal space. A helpful orientation is often an imaginary line from the tip of the scapula to the nipple. Transection of the subcutis on the rib with the monopolar knife. Subsequently, stepwise preparation of the intercostal muscles with the monopolar knife. The pleura is opened bluntly with fingers. Palpation of the thoracic wall for adhesions and insertion of a wound protection foil.
-
Access Uniportals VATS
![Access Uniportals VATS]()
-
Hilar Preparation
![Hilar Preparation]()
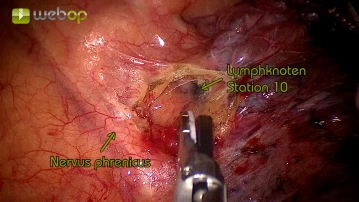
The operation begins with the preparation of the lung hilum. Initially, the pleural covering is incised, taking care to preserve the phrenic nerve. Subsequently, the pulmonary artery and the pulmonary veins can be gradually exposed through mostly blunt dissection (spreading or pushing).
A large lymph node from station 10 according to IALSCC (lung hilum) is exposed and should be removed even in non-oncological surgeries to facilitate further preparation at the hilum.
-
Preparation of the superior pulmonary vein
![Preparation of the superior pulmonary vein]()
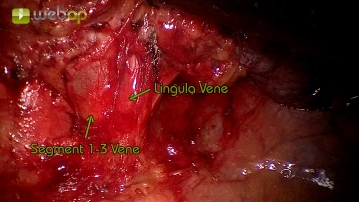
Now the upper pulmonary vein is circumferentially dissected free. The dissection is mostly blunt by spreading the tissue, situationally the perivascular tissue is transected with the ultrasonic scissors. The segments of the lingula (S4 and S5) often drain via a common trunk into the upper pulmonary vein. Before resection, the lingular vein is circumferentially exposed, as it must be preserved.
-
Preparation of the pulmonary artery
![Preparation of the pulmonary artery]()
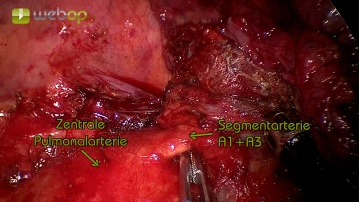
Representation of the central pulmonary artery through circular dissection of the perivascular tissue layer. This is also mostly bluntly resected, situationally using the ultrasonic scissors. Subsequently, the dissection is continued along the artery from central to peripheral until the segmental arteries are clearly visualized. The course of the segmental arteries in the left upper lobe is flexible and can often only be reliably assessed during the course of the operation. Common variants include a common arterial trunk of the segmental arteries A1 and A2 with another narrow-caliber branch of the segmental artery A3 or separate origins of the segmental arteries from the pulmonary artery.
-
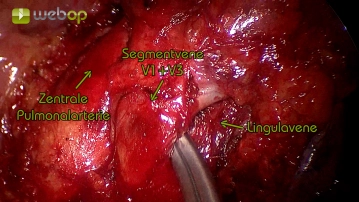
Dissection of the segmental veins V1 to V3
![Dissection of the segmental veins V1 to V3]()
After clearly displaying the confluence of the lingular vein (segments 4 and 5) in surgical step 3, the resection phase can now begin. Here, the common venous trunk of segments 1-3 is undermined using an Overholt and then transected with an endoscopic stapler.
Note:
- For narrow-caliber vessels, in addition to adequate dissection, a "Curved-Tip" cartridge of the stapler is helpful.
- Occasionally, traction on the vessel for preparation and insertion of the stapler can facilitate the maneuver.
Dissection of the segmental arteries A1 to A3
The first branch from the pulmonary artery is often formed from a common trunk of the segmental art
The first branch from the pulmonary artery is often formed from a common trunk of the segmental art
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
thoracic
Unlock all courses in this module.
€7.42
/ month
€89.00 / yearly payment