
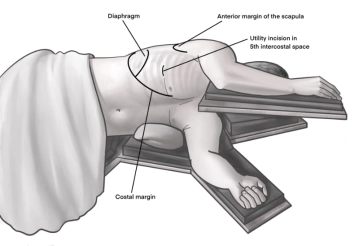
Incision of approximately 4 cm in length in the area of the anterior axillary line at the upper edge of the 5th rib to access the 4th intercostal space above. A helpful orientation is often an imaginary line from the tip of the scapula to the nipple. Transection of the subcutis on the rib with the monopolar knife. Subsequently, stepwise preparation of the intercostal muscles with the monopolar knife. The pleura is opened bluntly with a finger. Palpation of the thoracic wall for adhesions and insertion of a wound protection film.
-
Access uniportal VATS right
![Access uniportal VATS right]()
-
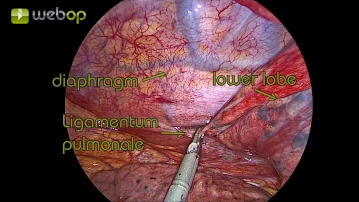
Preparation of the pulmonary ligament
![Preparation of the pulmonary ligament]()
First, the phase of lung mobilization follows. Using atraumatic grasping forceps or swabs, the lower lobe is pulled apically and the pulmonary ligament is dissected using an ultrasonic scalpel. During this process, the lymph nodes of station 9 according to IALSC (International Association for the Study of Lung Cancer) can be retrieved.
Note:
- Occasionally, it is necessary to press the diaphragm caudally with another swab. Care must be taken during positioning not to exert too much pressure on the abdomen, thereby causing diaphragmatic elevation and difficult surgical conditions.
-
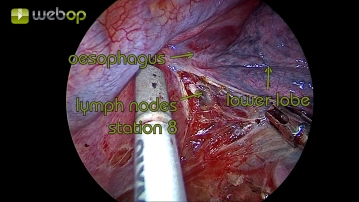
Preparation of the mediastinal pleura
![Preparation of the mediastinal pleura]()
The pleura extends circularly from the pulmonary ligament around the lung hilum cranially. To visualize the lung hilum, the lateral pleura is opened cranially along the resection line of the pulmonary ligament, and paraesophageal lymph nodes of station 8 (according to IALSC) are removed.
Note:
- Sometimes it is helpful, before further preparation of the central vessels, to dissect the fine pleural covering at the medial hilum between the aorta and lung and to achieve better mobilization and overview by blunt dissection.
-
Preparation of the lobar fissure
![Preparation of the lobar fissure]()
In well-developed interlobium, the dissection of the visceral pleura and smaller parenchymal bridges is performed using the ultrasonic scissors. Subsequently, the step-by-step exposure of the pulmonary artery is achieved. Accompanying lymph nodes of station 11 (according to IALSC) are directly retrieved to facilitate the preparation of the vessel and later dissection.
Note:
- The order of preparation, starting with the pulmonary artery or lower pulmonary vein, also depends on the situs. In the case of an obliterated lobar fissure and difficulties in exposing the pulmonary artery, prior resection of the vein may help gain better mobility and thus a better overview.
- After securely exposing the pulmonary artery, the parenchymal bridges can be transected using electrocautery, a stapling device, or a high-energy device.
-
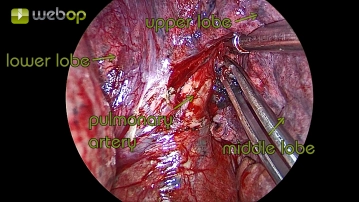
Preparation of the pulmonary artery
![Preparation of the pulmonary artery]()
After displaying the pars interlobaris of the pulmonary artery and resecting some lymph nodes for better visualization, the vessel must now be dissected to the extent that precise differentiation and visualization of the branching arteries is possible.
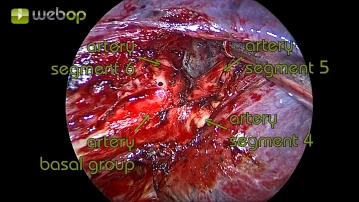
Resection of the basal part of the pulmonary artery
After clear identification, the pars basalis of the pulmonary artery, including the A6 segment arte
After clear identification, the pars basalis of the pulmonary artery, including the A6 segment arte
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
thoracic
Unlock all courses in this module.
€7.42
/ month
€89.00 / yearly payment