Positioning the patient on their back and padding the extremities as well as pressure-sensitive areas.
Positioning of both patient arms.
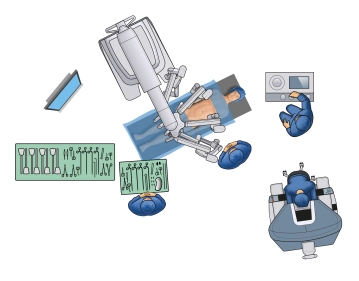
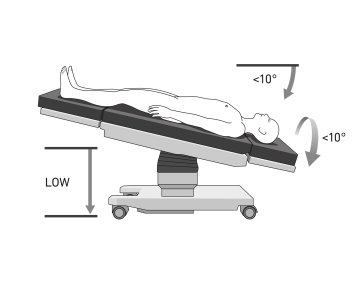
Positioning in 10° reverse Trendelenburg and 10° left lateral position, table as low as possible.
To maximize the reduction of positioning injuries and ensure safe positioning, positioning in the vacuum mattress is recommended.
Note: Positioning is particularly important due to the docking of the patient to the robot manipulator. The risk of injury to the abdominal wall when the patient slips must also be considered. With coupled tables in the Xi system, intraoperative position changes are possible without undocking. If the "Table-Motion" technique is not available, the surgical robot must always be undocked and removed from the operating table before any position change.
Caution: Vacuum cushions may have leaks. Therefore, they should be checked again before sterile draping.