
After infraumbilical transverse skin incision, expose the anterior rectus sheath with two Langenbeck retractors and incise it transversely with the scalpel. Retract the medial edge of the rectus muscle with the retractor and insert the dissecting balloon. Slides it on the posterior lamina of the rectus sheath to the pubic bone. Under direct vision with the 0° laparoscope, balloon dilation will bluntly dissect and thus help to clearly identify the guiding structures of the pubic bone, rectus muscle, and epigastric vessels. Remove the balloon and arm the incised anterior rectus sheath with braided size 0 absorbable sutures.
-
Access to the preperitoneal space
-
Inserting the laparoscope and first working trocar
Now, insert a Hasson trocar is inserted and securely fixed with the preplaced sutures. In most cases, a working pressure of 7 mmHg suffices to adequately unfold the preperitoneal space. Insert a 5 mm trocar at least 5 cm above the pubic bone in the midline.
Tip:
An insulated 5 mm trocar with short thread is recommended. -
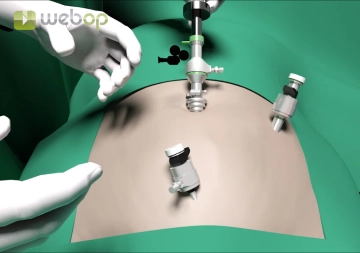
Dissecting the preperitoneal space and inserting the third trocar
![Dissecting the preperitoneal space and inserting the third trocar]()
While expand the medial preperitoneal space with the Overholt and laparoscope, the midline will be crossed. From here, the dissection proceeds laterad, with a large medial hernia readily apparent. Continue the lateral dissection along the transversus abdominis muscle to the level of the umbilicus. At this level in the anterior axillary line, insert the third trocar, either as a 5 mm or, as in the video, as a 10 mm trocar.
Notes:
- This position of the second working trocar allows good triangulation.
- Particular attention must be paid to the course of the lateral femoral cutaneous nerve during lateral preparation, especially when electrocoagulation is used.
-
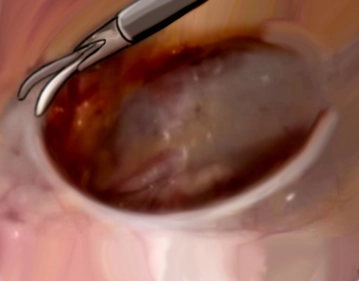
Freeing the hernial sac from the structures of the spermatic cord
![Freeing the hernial sac from the structures of the spermatic cord]()
Once all trocars have been inserted, the camera operator changes position and now stands behind the surgeon. Tilt the table to the side of the team; it often helps to tilt the table downward 10°.
Now detach the large direct hernial sac from the spermatic cord, identifying the ductus deferens and vessels, and dissect it sufficiently far craniad to allow for optimum mesh placement at a later stage. -
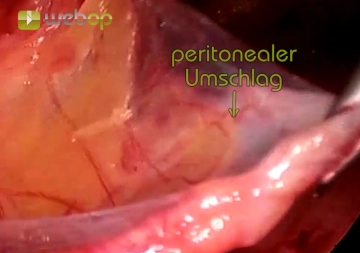
Dissecting off the peritoneum (parietalization)
![Dissecting off the peritoneum (parietalization)]()
If the arcuate linea extends far caudad, as in the video, it should be incised laterally. The final act of dissection is the dissection of the peritoneum off the spermatic cord or fascia beyond the middle of the psoas muscle toward the anterior abdominal wall. Divide all, even the smallest, fibrous attachments between the peritoneum and retroperitoneum. This will expose the inguinal nerves, the lateral femoral cutaneous nerve lateral to the psoas muscle and the genitofemoral nerve medial to the latter.
Gathering the transversalis fascia
Preperitoneal lipomas accompanying the structures of the spermatic cord should be mobilized far cr
Preperitoneal lipomas accompanying the structures of the spermatic cord should be mobilized far cr
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
general and visceral surgery
Unlock all courses in this module.
€12.42
/ month
€149.00 / yearly payment