1. Layer Structure
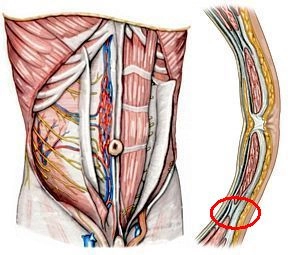
The large area covering the anterior abdominal wall from the xiphoid process or the costal arches to the pelvic bones has a typical layer structure: Beneath the skin and subcutaneous fat tissue, there are superficial fasciae, muscles and their fasciae, then an extraperitoneal fascia and the parietal peritoneum.
Especially in the anterior wall below the navel, the otherwise typical single-layered superficial fascia transitions into a two-layered structure (Panniculus adiposus abdominis) consisting of a superficial fat-rich layer (Camper's fascia) and a deeper membranous layer (Scarpa's fascia). The 5 abdominal muscles consist of:
3 oblique muscles (1. External oblique muscle, 2. Internal oblique muscle, and 3. Transverse abdominal muscle) and
2 straight muscles (4. Rectus abdominis muscle and the inconsistent 5. Pyramidalis muscle).
a) external muscle
Located immediately beneath the superficial fascia, it runs caudomedially to the large aponeurosis, both sides merging centrally into the linea alba. Its lower edge forms the inguinal ligament from the anterior superior iliac spine to the pubic tubercle, which in turn medially gives off the lacunar ligament and the pectineal ligament (Cooper).
b) middle muscle
Fibers run craniomedially, merging with fibers from 1. to the linea alba.
c) innermost muscle
Transversely running fibers, also radiating into the linea alba.
Each of the three oblique abdominal muscles has a thin, own fascia on its front and back surface, the transverse abdominal muscle on its inner side has the strong transversalis fascia. This lines the abdominal cavity and transitions cranially into the diaphragmatic fascia and dorsally into the thoracolumbar fascia. Caudally, it is attached to the iliac crest and transitions into the endopelvic fascia.
The rectus abdominis muscle is a long, straight, paired abdominal muscle, interrupted by 3 – 4 transverse tendinous intersections ("six-pack").
The pyramidalis muscle is a triangular, inconsistent muscle that originates from the upper pubic ramus and radiates into the linea alba. It lies ventral to the rectus abdominis muscle in its own sheath in the anterior layer of the rectus sheath.
2. Fasciae and Peritoneum
The rectus abdominis muscle and the pyramidalis muscle are enclosed by the rectus sheath, which is formed by the 3 oblique abdominal muscles. The rectus abdominis muscle is completely enclosed by it in its upper ¾, in the lower ¼ below the arcuate line only covered in front, while here the back surface of the rectus abdominis muscle only shows the transversalis fascia and the peritoneum. In the upper ¾, the anterior layer of the rectus sheath is formed by the external oblique muscle and half by the internal oblique muscle, the posterior layer half by the internal oblique muscle and the transverse abdominal muscle.
Between the transversalis fascia and the peritoneum is the extraperitoneal space, which can vary in thickness depending on location. In the retroperitoneum, the retroperitoneal abdominal organs are located here. On the anterior abdominal wall, it is repeatedly referred to as the preperitoneal space (e.g., at the internal inguinal ring).
The peritoneum (parietal serosa) forms the completely closed peritoneal cavity (exception: opening of the tube in women) and transitions as visceral peritoneum onto the intraperitoneal organs. Below the navel, it forms three folds:
the unpaired median umbilical fold (obliterated urachus/urinary duct)
the paired medial umbilical fold (former umbilical artery)
the paired lateral umbilical fold (inferior epigastric vessels).
3. Innervation and Blood Supply
The anterior abdominal wall is innervated by the anterior rami of the spinal nerves T7 to T11, T12 (subcostal nerve), and L1 (iliohypogastric nerve, and ilioinguinal nerve).
The superficial blood supply is cranially from the internal thoracic artery (→ musculophrenic artery), in the lower part from the superficial epigastric artery or the superficial circumflex iliac artery (both from the femoral artery). The deep blood supply comes cranially from the superior epigastric artery (← internal thoracic artery), laterally from intercostal vessels, and caudally from the inferior epigastric artery or the deep circumflex iliac artery (both from the external iliac artery). Venous drainage occurs via veins of the same name.