
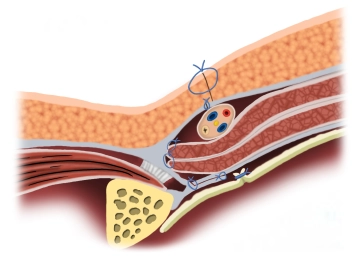
Duplication of the transversalis fascia and attachment of the transversus muscle and internal oblique muscle to the inguinal ligament for reconstruction and stabilization of the posterior wall of the inguinal canal.
-
Principle
![Principle]()
-
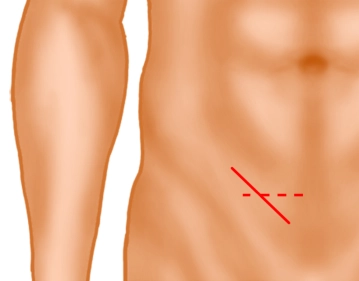
Inguinal skin incision
![Inguinal skin incision]()
A skin incision approximately 5 cm long is made obliquely two fingerbreadths above the inguinal ligament (solid line) or alternatively a transverse skin incision two fingerbreadths above the pubic bone. Subsequently, the subcutaneous tissue is incised down to the external oblique aponeurosis. Subcutaneously located superficial epigastric vessels are ligated (not shown).
-
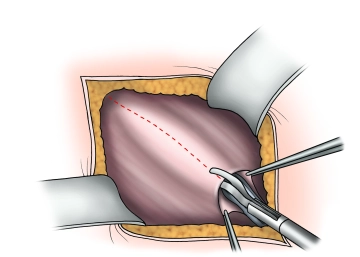
Splitting of the external aponeurosis
![Splitting of the external aponeurosis]()
The external aponeurosis is opened parallel to the fibers, including the external inguinal ring, extending beyond the level of the internal inguinal ring. The fascial edges are clamped, elevated, and the fascia is bluntly separated from the internal oblique muscle and the cremaster muscle.
Attention: The iliohypogastric nerve lies on the internal oblique muscle! -
Identification of the hernial sac; looping of the spermatic cord
The transversalis fascia is exposed up to the symphysis. After looping the spermatic cord at the level of the pubic tubercle, the spermatic cord is completely separated from the direct hernia sac.
Important: To avoid postoperative neuralgias, the following should be observed:
- If the genital branch of the genitofemoral nerve, the ilioinguinal nerve, or the hypogastric nerve cannot be preserved, the affected nerves should be resected and the resection ends infiltrated with a local anesthetic.
- Long stretches of nerve exposure and manipulation should be avoided. In case of doubt, it is better to perform a neurectomy than to leave a damaged nerve.
-
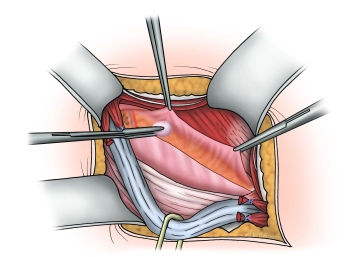
Division of the transversalis fascia
![Division of the transversalis fascia]()
The transversalis fascia is sharply incised from lateral to medial and bluntly separated from the underlying tissue. Care must be taken with the epigastric vessels to avoid bleeding.
The cranial lip should be generously mobilized, while the caudal lip should be mobilized minimally due to the risk of bleeding.
Note: Weak or thin fascial portions may be excised to obtain sutureable edges.
Shouldice Suture I
Continuous suture (non-absorbable thread 0/0 to 0/2) of the caudal edge of the transversalis fascia
Continuous suture (non-absorbable thread 0/0 to 0/2) of the caudal edge of the transversalis fascia
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
€7.99 inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from €3.70 / module
€44.50 / yearly payment
general and visceral surgery
Unlock all courses in this module.
€12.42
/ month
€149.00 / yearly payment