Ideally, the marking and subsequent instruction for stoma care should be performed by specially trained stoma therapists or an experienced surgeon.
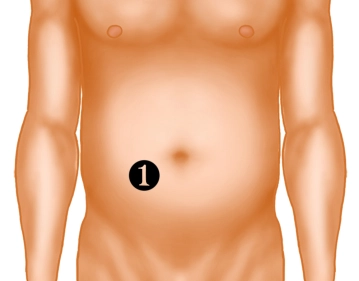
- Trial marking on the patient who is lying down or already seated in the area of the right rectus abdominis muscle (navel height) in a 10 × 10 cm skin area, preferably without folds, scars, or bony protrusions.
- Verification of the intended position in motion (standing, bending).
- The chosen site should be easily visible and accessible to the patient and should be compatible with the position of the pants or belt.
- Determining an alternative marking is recommended in case of intraoperative complications.
- Covering the marking with a skin-friendly adhesive tape.
The position of the stoma significantly influences handling and care, and thus the patient's quality of life!