
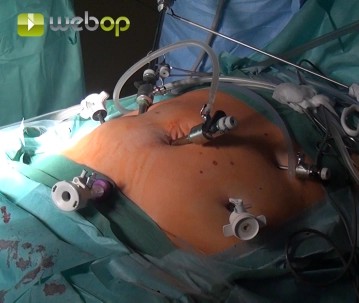
Due to obesity and a periumbilical scar, the pneumoperitoneum is established with the Veress needle subcostally on the left. First, in the right mid-abdomen, a channel for a 10mm trocar is bluntly created with scissors and placed. Now, under direct vision, another 10mm trocar is introduced umbilically and a 5mm trocar is inserted into the right lower abdomen. Through this, adhesions to the median umbilical ligament close to the abdominal wall up to the bladder are initially released. Subsequently, a 12mm trocar can be introduced suprapubically in the area of the planned Pfannenstiel incision. Two additional 5mm trocars are placed in the left mid and upper abdomen, with the latter utilizing the insertion site of the Veress needle.
-
Puncture Pneumoperitoneum; Placement of Trocars
![Puncture Pneumoperitoneum; Placement of Trocars]()
Soundsettings -
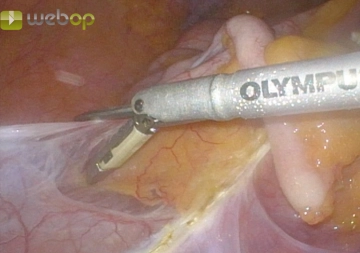
Preparation of the Ileocecal Transition
![Preparation of the Ileocecal Transition]()
Soundsettings First, the terminal ileum, cecum, and ascending colon are mobilized from below and laterally, respecting the Gerota's fascia.
Note: During the preparation of the right hemicolon, the surgeon and first assistant stand on the patient's left side, facing the monitor on the patient's right side. From the preparation of the left hemicolon (step 7) until the end of the operation, the sides are switched, and a second monitor is set up on the patient's left side.
-
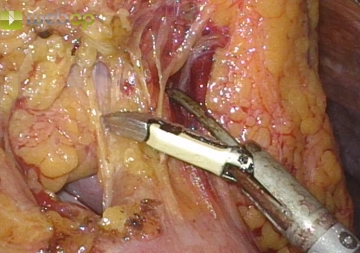
Mobilization of the Ascending Colon with Detachment of the Right Flexure
![Mobilization of the Ascending Colon with Detachment of the Right Flexure]()
Soundsettings The mobilization of the ascending colon with the mesenteric root up to the duodenum on the Gerota's fascia is completed under free preparation of the duodenum. In this process, the right colonic flexure is dissected from the side and above, with adhesions to the gallbladder and a double-barrel formation between the ascending colon and the transverse colon being severed.
-
Detachment of the Greater Omentum
![Detachment of the Greater Omentum]()
Soundsettings Now the gastrocolic ligament is transected while opening the omental bursa. The greater omentum remains in situ and is dissected from the transverse colon from left to right.

Division of the Ileocolic Vessels
In a vessel-free window between the middle colic artery and the ileocolic artery, the mesocolon is
In a vessel-free window between the middle colic artery and the ileocolic artery, the mesocolon is
Activate now and continue learning straight away.
Single Access
Activation of this course for 3 days.
US$9.20
inclusive VAT
Most popular offer
webop - Savings Flex
Combine our learning modules flexibly and save up to 50%.
from US$7.14 / module
US$85.75/ yearly payment
general and visceral surgery
Unlock all courses in this module.
US$14.29
/ month
US$171.50 / yearly payment
Webop is committed to education. That's why we offer all our content at a fair student rate.